
Modern interventional cardiology
19 July 2015
Interventional cardiology (also: invasive cardiology) refers to diagnostic and therapeutic cardiac interventions that can be performed using catheters. Today, interventional cardiology occupies a leading position in the treatment of cardiovascular diseases and contributes to the fact that the mortality of patients with diseases such as myocardial infarction, severe heart failure or valvular heart disease is steadily decreasing.
Interview with Prof. Dr. Wenaweser

Prof. Dr. med. Peter M. Wenaweser - Interventional Cardiology - HerzKlinik Hirslanden
What options does interventional cardiology offer?
In interventional cardiology, new methods have been developed in recent years that have revolutionized treatment options. Depending on the clinical picture, a specific vascular access is chosen through which the catheters are introduced.
Interventional cardiology techniques are an important cornerstone of the treatment of cardiovascular diseases and complement advances in rhythmology, in the treatment of heart failure and in cardiac surgery and drugs. Thanks to these advances, it is becoming increasingly possible to offer patients high-quality, minimally invasive therapy.
What is the procedure for intervention via the wrist artery (radial artery)?
With catheters (2-3 mm in diameter) inserted via this access (see figure a), most examinations and interventions on the coronary arteries can be performed. Balloon dilatation (PTCA, dilatation of a narrowed coronary artery) is still the most common procedure in interventional cardiology and enables rapid and safe treatment of coronary artery disease by means of stent implantation (vessel support). Currently, drug-eluting stents (DES) are routinely used because they have a very low rate of reocclusion (restenosis). Newer stent technologies such as resorbable stents (BVS), which dissolve over time, are only being used selectively and have yet to compete with established DES in trials and in clinical practice. The elegant access via the wrist artery allows the patient to get up immediately after the procedure and leave the hospital the same day. In addition, the risk of bleeding is lower than with access via the inguinal artery.
Intervention via the inguinal artery (femoral artery)?
The inguinal artery (see figure b) is the standard access for complex interventions on the coronary vessels and, thanks to the larger vessel diameter, offers more possibilities to perform highly specialized interventions. This access is particularly important for the treatment and clarification of valvular heart disease. Minimally invasive aortic valve replacement (TAVI) is a routine procedure at specialized centers and is superior to open heart surgery in selected patients. Prerequisite for a successful application are detailed preliminary examinations with ultrasound and other imaging techniques (computer tomography). The majority of TAVI can be performed without general anesthesia. For the remaining patients, access via the apex of the heart (transapical - see figure d) or introduction of the system via the subclavian artery (see figure c) can be considered. Furthermore, interventions on the leg, neck or renal vessels can also be performed via the inguinal artery.
Intervention via the inguinal vein (femoral vein)?
Interventions via venous access (see figure e) are in principle less prone to complications due to the lower pressure compared to the arterial area. Typically, it is used for blood flow measurements (hemodynamic measurements), tissue sampling (myocardial biopsies), and evaluation of pulmonary pressure. This approach is also used to close or treat congenital heart defects (shunt vitias) such as atrial septal defect (ASD) or persistent foramen ovale (PFO), an open connection from the right to the left atrium. Such a connection carries the risk of circulatory overload or heart failure, as well as thrombotic complications that can lead to a stroke: Small clots that have formed in the leg veins are not intercepted in the pulmonary circulation, but enter directly into the arterial circulation and, in the worst case, block a cerebral artery. With a so-called umbrella implantation, such defects can be easily repaired - without heart surgery.
Transseptal puncture: intervention via the cardiac septum?
Venous access is also used to perform a transseptal puncture (piercing the cardiac septum). This deliberately creates a connection between the right and left atrium, allowing interventions on the mitral valve, the valve between the left atrium and the left ventricle, such as balloon dilatation of a narrowed valve or the catheter procedure for a leaking valve (Mitra clip). In high-risk patients with severe leakage of the mitral valve, the Mitra clip procedure has become established as a good alternative in recent years. The leakage is closed with a clip. For successful application, ultrasound technology and fluoroscopy technology have to be combined. The hybrid operating room offers the optimal conditions for this. As with TAVI procedures, this also requires a highly specialized team.
In addition, transseptal puncture can also be used to occlude the left atrial appendage (LAA), which is a niche for clot formation in patients with atrial fibrillation. This newer technique involves the cardiologist closing the left atrial ear with an implant. This eliminates the major source of embolism and reduces the risk of stroke. In particular, patients who are taking blood-thinning therapy for atrial fibrillation and are prone to bleeding benefit from atrial appendage closure. After closure, long-term therapy with aspirin alone is possible.

Schematic of diagnostic and therapeutic approaches in interventional cardiology:
a Wrist artery (radial artery) for
1 Coronary arteries (balloon dilatation / stenting)
b Inguinal artery (Arteria femoralis) for
1 coronary artery (balloon dilatation / stenting), 2 aortic valve (TAVI), 3 renal artery, 4 carotid artery
c subclavian artery, for 2 aortic valves (TAVI)
d Transapical approach, for
2 Aortic valve (TAVI)
e inguinal vein (Vena femoralis), for
5 Cardiac septum / foramen ovale (umbrella device / blood flow measurement / transseptal puncture), 6 Mitral valve (reconstruction / mitral clip), 7 Left atrial tube (closure) and 8 Myocardium (biopsy)
More reports

Gentle heart surgery with the DaVinci robot
Interview with Prof. Dr. med. Jürg Grünenfelder The DaVinci surgical robot is mainly known from the field of prostate surgery. In the...

New clip procedure on the tricuspid valve
Switzerland's first use of a new clip procedure on the tricuspid valve On February 20, 2018, a team from HerzKlinik Hirslanden in...

Every heart loves movement
Interview with Prof. Christophe Wyss, MD Many factors influence heart health. Cardiologists agree: sport and exercise do...
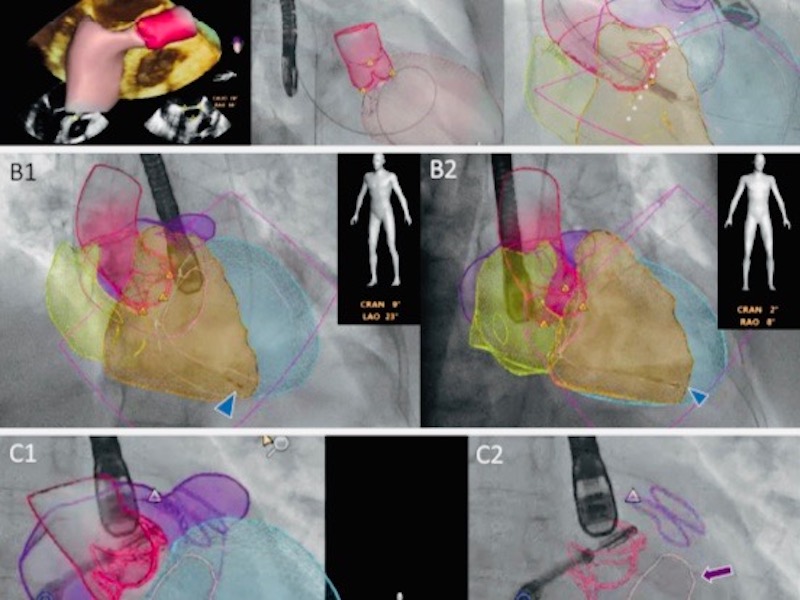
Cardiac imaging with echocardiography and fluoroscopy (Heart Imaging)
Automated anatomical intelligence: next-generation fusion imaging in structural cardiac interventions Cardiac teams performing structural cardiac interventions face particular imaging difficulties,...
TAVI catheter for aortic valve replacement
Aortic valve replacement: surgical or catheter-based using TAVI Once developed for high-risk patients, this method of aortic valve replacement is increasingly being used in patients with...

Heart attack - Yes or No?
Chest pain has different causes, but what they all have in common is that they frighten the sufferer. Although up to 90% of the symptoms can be...
All specialists at the Heart Valve Center of Herzklinik Hirslanden
Prof. Dr. med. ROBERTO CORTI
Interventional Cardiology
Prof. Dr. med. JÜRG GRÜNENFELDER
Cardiac Surgery
MD. THIERRY AYMARD
Cardiac Surgery
PD Dr. med. PATRIC BIAGGI
Cardiology | Imaging
Prof. Dr. med. OLIVER GÄMPERLI
Interventional Cardiology
PD Dr. med. DAVID HÜRLIMANN
Cardiology | Rhythmology
Dr. med. IOANNIS KAPOS
Cardiology | Imaging
MD. SILKE WÖRNER
Cardiology | Imaging
Prof. Dr. med. GEORG NOLL
Cardiology | Prevention
MD. IVANO REHO
Cardiology | Aortic Aneurysm
PD Dr. med. (H) DIANA RESER
Cardiac Surgery
Prof. Dr. med. JAN STEFFEL
Cardiology | Rhythmology
Prof. Dr. med. PETER M. WENAWESER
Interventional Cardiology
Prof. Dr. med. CHRISTOPHE WYSS
Interventional Cardiology